PRP Preparation: Open or Closed Technique?
- Feb 21, 2023
- 5 min read
Doctors have recently discovered that the body is capable of healing itself. A type of regenerative medicine known as platelet-rich plasma (PRP) treatment can take advantage of these properties and boost the natural growth factors your body produces while healing tissue. The development of PRP products to stimulate tissue repair and regeneration has been an important research field in biomaterial and pharmaceutical sciences for decades. The tissue healing cascade incorporates many players, including platelets with their growth factor and cytokine granules, leukocytes, fibrin matrix, and many other cytokines, which work synergistically.
The biology of PRP concentrates is as complex as blood itself and likely more complex than traditional pharmaceutical drugs. PRP products are living biomaterials, and the outcomes of clinical PRP applications are dependent on the intrinsic, versatile, and adaptive characteristics of the patient’s blood, including various other cell constituents that may be present in the PRP specimen and the interaction with the recipient local microenvironment, which can be in an acute or chronic state.
Preparation of PRP
A study by IADVL created a comprehensive literature search and found that there are numerous methods of PRP preparation. However, all of them primarily involve differential centrifugation and classified them into 2 categories.
2 two primary methods of PRP preparation:
1. Open technique: This method involves the open preparation of PRP. The blood encounters the environment in the working area. Pipettes and tubes are sterilised separately and used in the process of preparation of PRP.
2. Closed technique: This method involves the use of commercial devices or kits. Here the blood or the PRP is not exposed to the environment during the process of preparation of PRP.
Open Method
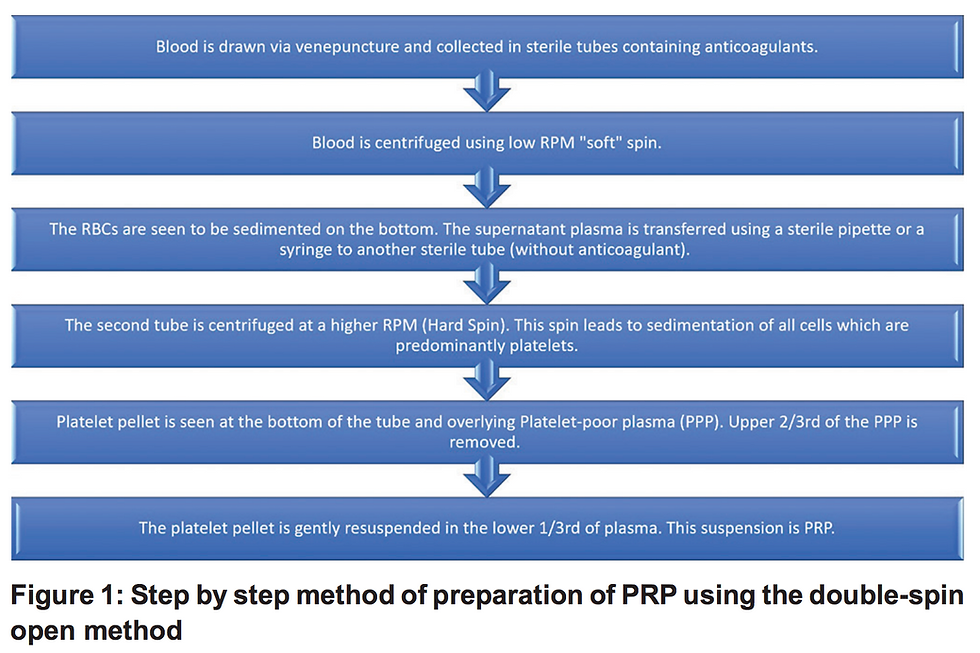
The double‑spin open method of preparation of PRP has been shown in the framework below. The first spin sediments the heavier Red blood cells (RBCs). The liquid supernatant is transferred to another tube and centrifuged again. The second spin is a higher RPM spin which pellets the platelets and the remaining cells. The top two‑thirds of the cell‑free supernatant after the second spin is discarded and the cell pellets are resuspended in a smaller volume of plasma.
The double‑spin open method is the preferred method of preparation for dermatologic needs due to its low cost, good platelet yield, and versatile volume of PRP production. (Quality of Evidence: High; Strength of recommendation: Strong)
The position of supernatant transfer after the first spin determines the type of PRP produced. For the preparation of pure PRP (P‑PRP), only the supernatant along with the top buffy coat is transferred to the second sterile tube for the second spin. Similarly, to prepare leukocyte‑rich PRP (L‑PRP), we need to transfer the complete supernatant along with the entire buffy coat and some RBCs to the second sterile tube.
A study suggested an innovative and economical method for the preparation of PRP—the syringe‑only method. They recommend a simple modification of a 5 mL syringe that allows its insertion into the centrifuge. The syringe is inserted piston down into the centrifuge. After separation, the supernatant is transferred to a different syringe using a 3‑way canula for the second spin. The advantage of this method is that it is a closed method where the blood product remains inside commonly available medical disposables like 3‑way canula and syringes, which are even approved for intravenous injections. (See figure below)

Another innovative method described in the literature is the turn‑down turn‑up method to prepare PRP. This method needs only one 10 mL syringe and two vacutainers, preferably 8.5 mL. It is a double‑spin method where vacutainers are placed in an inverted position for the first spin and the correct position for the second spin. This method has the drawback of having a high hematocritor RBC‑containing PRP. (See figure below)

A limitation of PRP produced using the open method is the risk of contamination of PRP. This can be minimised by preparing the PRP using all aseptic precautions with preparation preferably done under laminar airflow. A face mask, sterile disposable gloves, and a sterile gown are a must for the physician preparing the PRP as handling of blood products to prevent infection. PRP has been found to have strong antimicrobial activity. Studies have found a strong antimicrobial activity of PRP against methicillin‑resistant Staphylococcus aureus (MRSA) and Group A Streptococci. Both these studies have used pure PRP and not L‑PRP hence leukocytes did not play a role in the bactericidal activity of PRP.
Closed Method
Closed systems do not expose the platelets to the external environment after the process of blood collection. This system involves the use of a commercial kit paired mostly with a complementary centrifuge machine. And while most of these kits are marketed with Food and Drug Administration (FDA) ‘labels,’ it would be pertinent to understand that these approvals are simply for device safety (510 [k] approval) and not for efficacy.
The classification takes the following parameters into account: Dose of injected platelets (yield), efficiency or recovery of platelets during the process, purity of platelets, and activation. The dose of platelets injected was the total number of platelets in the final PRP produced (concentration of platelets × volume of PRP) measured in billion platelets. The efficiency of platelet recovery was calculated as a percentage of original platelets that were recovered in the final PRP product. The purity of platelets measured the contamination of platelets by other cell types. It measured the percentage of cells that were platelets out of all the cells in the PRP and finally if the PRP was activated or not.
The classification then gives ranks to the different methods of preparation of PRP from A to D, A being the best. An interesting observation that comes from this classification is that methods that have a higher dose of platelet, do not produce a pure PRP. This indicates that the purity of PRP may be inversely related to the number of platelets captured. Double‑spin open system (homemade in the classification) may be the recommended method of preparation of PRP which has received good scores on all parameters, is easy to prepare, and is cost‑effective.
Conclusion
The science behind the preparation of PRP is still in its infancy. We are far from producing the ‘ideal’ PRP and using this autologous biological product to its fullest potential. There are multiple pitfalls that one must avoid while preparing PRP. It is critical for the practitioners to be aware of the different facets of PRP preparation to ensure that they deliver the best therapeutic result to their patients.
Reference
Preparation of Platelet-Rich PLasma: National IADVL PRP Taskforce Recommendations (2021)
A new Economic Method for preparing platelt-rich plasma (2014)
CoDEPA classification: A proposal for standardising PRP use and a retrospective application of available devices (2016)
Classification Systems for Platelet-Rich Plasma (2019)
Uncovering the techniques of damaged skin regeneration & reparation in our upcoming
Advanced PRP (Platelet Rich Plasma) Therapy Hands-On Master Classes/Mini Fellowship happening globally:
IFAAS Hands-on Master Class/Mini Fellowship (Hands-On)
Advanced PRP (Platelet Rich Plasma) Therapy
For Facial, Neck, and Hair Rejuvenation
March 3, 2023 - Sydney, Australia - [Register Now]
More Upcoming Aesthetic Trainings Happening Globally
Comments